The day was windy. Extremely windy. Reports were coming in of metal roofing being torn off and landing on power lines at the Showgrounds shutting down Howitt Street near Creswick Road. My weather app indicated peak wind gusts of 93 kilometres per hour.
I was running late for my appointment, my heart rate was already up and I was agitated. Not a great way to attend my cardiac stress test. Ringing the diagnostic centre to tell them I would be running late, the staff thanked me to letting them know.
Having recently been suffering chest discomfort and with a familial history of heart problems on my fathers side, I had talked with my doctor about getting some tests done. The blood work up didn’t find anything significant although my Low Density Lipids (LDL) reading was up. Recently I had been under increased stress particularly in relation to our Bushfire earlier this year and this might have been the cause. We agreed that a cardiac stress test might be in order.
So on this windy, turbulent Friday I finally arrived bang on time at the diagnostic centre. I missed the fifteen minute arrival window but they were busy anyway. The form had said 2:45pm for a 3:00pm appointment.
After checking in, I sat comfortably in the waiting room. To fill in time, I scanned the news feeds for information about the storm. Just after 3:30, I was collected by a nurse who guided me into a consulting room. “Have you had one of these before?” she asked. “No,” I answered feeling surprisingly unphased by the experience. She gave me a quick run down on the procedure and said she would need to prepare me with the little sticky dots from which the readings would be collected.
The test would involve taking my blood pressure, 12-lead echo cardiograms, and ultrasound images of my heart. Once the initial, or baseline, information was collected, I would be placed on a treadmill that would increase in speed and inclination until I reached the target heart rate, I suffered chest discomfort, or the staff were satisfied no problems were occurring. “How long will this take?” I asked. “Usually no more than 20 minutes,” she replied. She quickly took my height and weight, scribbling them into her notes.
She broke out a brand new razor and I chuckled. There isn’t a lot of hair on my body but she said it was necessary to ensure that the dots would have uninterrupted contact with my skin. “This would avoid any unnecessary artifacts,” she said. Artifacts meaning false readings or noise that might reduce the accuracy of the measurements.
Having given me a cursory scraping, she disposed of the razor and attached the little sticky patches at twelve designated spots around my body. Mostly on my front, I was interested to note that she attached two on my lower back; widely set apart and just above my pelvis. The others were of no real surprise to me; both sides at the top of my chest, over my heart in a few places, and on my left side below the rib cage. The recording device was strapped around my waist and the leads clipped to the dots to begin collecting data. She was kind enough to take a couple of pictures

There was short delay as the person before me was “fit and this might take a while.” However just before 4:00pm, I was called in. The two technicians introduced themselves and one of them began by hooking up the recorder to the main device where it downloaded the collected data into my central records. He agreed to take more pictures of the test so that I could present them here. My blood pressure was also taken.
Satisfied that current recordings were being collected, he rolled me onto my left side and began taking some ultrasounds. This is not a gentle process but it isn’t exactly painful either. Each measurement required me to take a breath which had to be neither too shallow nor too deep then hold it. It was a bit of a struggle to hold the air in but I got there in the end. The probe appeared to be placed between the fifth and sixth rib on my left side, and just to the left side of my sternum.
At this point, the cardiologist came in and introduced himself. Asking the relevant recent history (Hx), and past and family history (PHx) questions helps build the wider picture leading up to the testing procedure. My family history and the recent chest discomfort seemed to make this procedure relevant on the day. I know as a man, with a high pain tolerance too, I tend to underplay my various maladies but my years of in-field experience reminded me how important it was to preclude the more serious reasons for what I had been feeling.
I was moved across to the tread mill where the second technician again explained the process. The treadmill would start off at a slow speed and on a flat plane. Every few minutes the speed and incline would increase while they would monitor my responses. Activating the treadmill, the pace was nice and easy however I suddenly realised they were firing questions at me. These were designed to increase the pressure on me mentally while my body was being challenged as well.
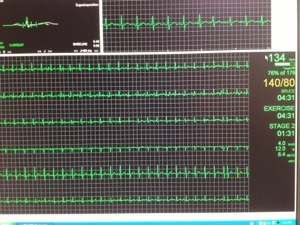
At regular intervals my blood pressure would again be monitored and this data was tagged against the ECG readings. I guess the treadmill process had taken about fifteen minutes when the first technician told me that when it stopped, I would need to slow down with the machine before hopping off then I would need to move straight back to the bed where more measurements would be taken. However there could be no delays as he only had 60 seconds to collect the next set of ultrasounds.

While I was only mildly out of breath, it was very hard to hold my breath for the next set of images. The cardiologist and the technician discussed which information to use and I was invited to look at the comparisons between the before and after recordings. It is somewhat disconcerting if fascinating to watch the valves of my heart fluttering in motion. The differences were explained to me and I could clearly see the left ventricle having expanded in volume to compensate for the increased demand by my body for oxygenated blood.
The outcome of the day was the opinion by the cardiologist that there were no major blockages although minor ones would not be apparent with this level of testing. Further assessments of the day’s data would be made before the final report would be issued to my doctor.
I was pleasantly surprised to see only half an hour had elapsed since I had entered the room and I was leaving no increased discomfort. My phone had a range of images and a few short videos of the whole process courtesy of my friendly technicians.
The final outcome is yet to be provided but at least the worst possible problem appears to have been discounted.
Chest discomfort or pain should never be ignored. Catching problems early may prevent a potentially fatal heart attack and certainly improve outcomes in the longer term. Changes in diet, activity and lifestyle may be necessary but they are achievable. A couple of things for me to take on board are that a) I need to lose some flubbed around the middle and b) my life could be improved by increasing my physical exercise for increased cardio capability.
What do you think you could do to improve your lifestyle? What are the signs and symptoms of a cardiac emergency? Not sure? Contact Key2Act to arrange some first aid training.
Like this:
Like Loading...